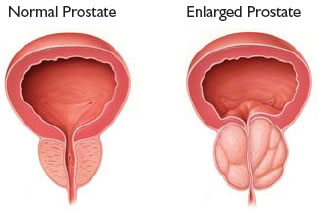
BPH is an acronym for the condition known as benign prostatic hyperplasia or what is commonly referred to as prostate enlargement. Oftentimes, patients confuse BPH with prostate cancer. As the name of this condition implies this is a benign condition and is not associated with malignant or cancerous prostate conditions.
BPH is diagnosed by your physician after performing a complete history and physical examination. The symptoms of BPH coupled with a rectal examination demonstrating an enlarged prostate is suggestive of the condition. Your physician might ask you to fill out a questionnaire quantifying the degree of your symptoms. The IPSS (International Prostate Symptoms Score) is a validated questionnaire utilized by physicians to quantify the degree of BPH symptoms. Your physician will have to perform some tests to confirm your condition. Additional tests include: PSA and Testosterone, Urine analysis and culture to rule out urinary tractinfection, Residual urine determination, Flow rate, Cystoscopy, Transrectal ultrasound, Urodynamics.
What are the available medical treatments for BPH?
There are several medications available for the treatment of BPH. These medications can be divided into three general categories: phytotherapy, alpha-blockers and 5-alpha reductase inhibitors.
Phytotherapy
Saw palmetto is an extract from the berry of the dwarf palm that is indigenous to the Southeastern United States. It is a non-prescription medication available at most drug stores and its production and distribution are not regulated by the FDA. It is usually taken at a dose of 160 mg twice daily. Despite its popularity, the medical literature has not shown this medication to have any benefit over placebo medications. A recent randomized double blind placebo controlled study showed that saw palmetto has no benefit in relieving prostate symptoms or objective parameters of BPH compared to placebo.
(Bent S et al, N Engl J Med, February 2006)
Alpha-Blockers
Alpha blocker medications are drugs that block the alpha receptors in the prostate causing relaxation of the smooth muscle component of the prostate. This relaxation allows the channel to open and relieves a man of his urinary symptoms. Alpha blockers can be divided into two different categories: selective and non-selective. The non-selective alpha blockers, as the name implies, are not specific for the prostate and can effect other organ systems. The effects on other organ systems can cause decreases in a man’s blood pressure, dizziness, runny nose, sexual dysfunction and erectile dysfunction. These non-selective alpha blockers also require dose titration to prevent the most severe of these side effects. Non-selective alpha blockers include terazosin, prazosin and doxazosin.
In contrast, the selective alpha blockers are designed to exert their effect primarily on the prostate. Medications such as tamsulosin (Flomax) and alfuzosin (Uroxatrol) are the two FDA approved selective alpha blockers. These medications have been shown to be equally effective to the highest doses of the non-selective alpha blockers while minimizing the side effects of this medication class.
5-alpha Reductase Inhibitors (5ARI)
The prostate gland grows under the direct influence of testosterone. The drug class of 5ARI’s prevent the conversion of testosterone to dihydrotestosterone (DHT), the more potent form of testosterone which has its primary effect on the prostate, liver and scalp. By suppressing the amount of DHT, we can decrease the size of the prostate gland by “starving” the gland.
There are two FDA approved medications in the 5ARI class: finasteride (Proscar) and dutasteride (Avodart). The difference between the two drugs is that dutasteride inhibits both types of 5ARI in the prostate, whereas, finasteride only inhibits one of the isoforms. This translates to a 97% vs 70% effectiveness of inhibiting 5ARI, respectively. Both medications are fully effective after 6 continuous months of therapy and cause a decrease in the PSA by at least 50%.
Combination Therapy
Combination therapy with an alpha blocker and 5ARI has been shown to be the most effective medical therapy for BPH. Combination therapy is usually reserved for men with progressive symptoms on monotherapy.
What are the available surgical treatments for BPH?
Minimally Invasive Treatments
Catheterization
Placement of a catheter into the bladder will temporarily drain urine. Catheters can be placed intermittently every six to eight hours—clean intermittent catheterization—or left in place for one to three months at a time (indwelling). Catheters can be placed either through the urethra or by making a small puncture into the bladder above the pubic bone (called a suprapubic tube). Infection is the biggest risk of having a catheter in place for long periods, as bacteria can stick to the surface of the catheter, making it difficult for the body’s immune system or antibiotics to clear the organisms. Another risk is that after a few years there is a higher risk of bladder cancer due probably to the long-term irritation caused by the catheter sitting in the bladder. Catheterization, performed by the individual or a caregiver every six to eight hours, minimizes the risk of infection and cancer compared with an indwelling catheter. Catheters are most useful as a treatment of choice for temporary drainage while waiting for medication to start working, surgery to be scheduled, or clearance of infection. They also might be the most appropriate choice for a patient with multiple medical problems and a short life expectancy, where the risk and discomfort of surgery outweigh the risk of infection or cancer. Catheterization is the treatment of choice over medications or surgery for patients who have neurogenic bladder in addition to prostatic obstruction.
Microwave Thermotherapy (TUMT)
This is an office-based procedure performed with topical and oral pain medication and does not require anesthesia. Computer-regulated microwaves are sent through a catheter to heat portions of the prostate. A cooling system is required in some types for better tolerance. Traditionally, the best use of this procedure has been for patients who have too many medical problems for more invasive surgery or for patients who truly wish to avoid any type of anesthesia. Benefits are that there is no need for anesthesia and there is no blood loss or fluid absorption (these would be significant benefits in a person with a weak heart). Patients usually go home the same day. Many urologists have the technology available in their practice and results are pretty reliable regardless of who performs the procedure. The use of TUMT has been expanding to a broader patient population and there are several types of TUMT machines available.
TUNA
The procedure involves anesthesia and medications to make the patient sleepy. The technology involves heating of tissue using radio frequency energy transmitted by needles inserted directly into the prostate. High frequency radiowaves heat the prostate up to very high temperatures. The heated prostate tissue is destroyed and initially swells but then shrinks. Most men require a catheter for a period of time after this procedure. Advantages in the use of TUNA include the limited anesthesia requirement, the ability to perform the procedure in an office setting and avoidance of serious complications sometimes associated with other procedures.
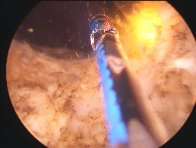
Photoselective Vaporization of the Prostate (PVP)
This is fast becoming a very popular procedure performed either in a well equipped office or as an out-patient at the hospital. It uses a high-powered laser that vaporizes the obstructing prostate tissue with minimal bleeding or side effects. This procedure can serve to get men off of medical therapy. It is effectively replacing more invasive surgical treatment.
Transurethral Resection of the Prostate (TURP)
Transurethral resection is the most common surgery for BPH. In the United States, approximately 150,000 people have TURPs performed each year. This can be done using electric current or with laser light. After the patient receives anesthesia, the surgeon inserts an instrument called a resectoscope through the tip of the penis into the urethra. The resectoscope contains a light, valves for controlling irrigating fluid and an electrical loop that cuts tissue and seals blood vessels. The removed tissue pieces are carried by the irrigating fluid into the bladder and then flushed out and sent to a pathologist for examination under a microscope. At the end of the procedure, a catheter is placed in the bladder through the penis. The bladder is continuously irrigated with fluid through the catheter in order to monitor bleeding and prevent blood from clotting and obstructing the catheter. Since there are no surgical incisions with this procedure, patients normally stay in the hospital only one to two days. Depending on surgeon preference, the catheter may be removed while the patient is still in the hospital or the patient may be sent home with the catheter in place, attached to a leg bag for convenience and removed several days later as an outpatient procedure.
Transurethral incision of the prostate (TUIP)
Transurethral incision is used for men with smaller prostate glands who suffer from significant obstructive symptoms. Instead of cutting and removing tissue to relieve the obstructed bladder, this procedure widens the urethra by making several small cuts in the bladder neck where the urethra joins the bladder and in the prostate itself. This reduces the pressure of the prostate on the urethra and makes urination easier. Patients normally stay in the hospital one to three days. A catheter is left in the bladder for one to three days after surgery.
Open Surgery – Simple Prostatectomy
When a transurethral procedure cannot be done, open surgery may be required. Open prostatectomy for BPH is also performed for a prostate that is too large to remove through the penis. Other reasons for choosing an open prostatectomy include patients with large bladder diverticula, with large bladder stones and who cannot physically tolerate having their legs placed in stirrups for TURP/TUIP surgery.
An incision is made in the abdominal wall from below the belly button to the pubic bone. The prostate gland can then be removed in its entirety through either an incision in the fibrous capsule surrounding the prostate (retropubic prostatectomy) or through an incision made in the bladder (suprapubic prostatectomy). Postoperative pain is mild to moderate. Patients usually stay in the hospital for several days and go home with a urinary catheter. In some cases a second catheter draining the bladder through the lower abdominal wall is used.
Postoperatively, patients typically experience significant improvement in their symptoms (table 1). As with any operative procedure, complications do exist. Some occur in the early postoperative period (table 2) while others may occur many years later (table 3).
Table 1: Overall improvement in patient symptoms
TURP
TUIP
Open
88%
80%
98%
Table 2: Immediate post-operative complications
TURP
TUIP
Open
Infection
15%
13%
13%
Bleeding Requiring Transfusion
5-10%
1%
8%
Impotence
14%
12%
17%
Retrograde Ejaculation
73%
25%
77%
Incontinence
1%
<1%
<1%
Table 3: Late post-operative complications
TURP
TUIP
Open
Stricture and bladder neck contracture
(scar tissue causing obstruction)
Will surgery for BPH affect my ability to enjoy sex?
Most urologists say that even though it takes a while for sexual function to return fully, most men are able to enjoy sex again. Most experts agree that if you were able to maintain an erection shortly before surgery, you will probably be able to do so after surgery. Most men find little or no difference in the sensation of orgasm although they may find themselves suffering from retrograde ejaculation.






 BPH is an acronym for the condition known as benign prostatic hyperplasia or what is commonly referred to as prostate enlargement. Oftentimes, patients confuse BPH with prostate cancer. As the name of this condition implies this is a benign condition and is not associated with malignant or cancerous prostate conditions.
BPH is an acronym for the condition known as benign prostatic hyperplasia or what is commonly referred to as prostate enlargement. Oftentimes, patients confuse BPH with prostate cancer. As the name of this condition implies this is a benign condition and is not associated with malignant or cancerous prostate conditions.